What is CTE?
When people hear the three letters “CTE”, many immediately think of the highly publicised American cases linked to professional sport. Media coverage in the United States focused heavily on former NFL players and the devastating consequences of repeated head impacts, often framing the issue through stories of crime, tragedy and extreme outcomes. These narratives, while attention-grabbing, have sometimes overshadowed the wider and more complex reality of brain injury.
Alongside this coverage came a landmark legal case against the NFL, brought by more than 4,500 former players. They alleged the league failed to adequately inform or protect them from the long-term effects of concussions and repeated head trauma. The case was settled out of court in 2013 for $765 million, without an admission of liability, but it marked a turning point in how sport began to confront brain health.
Similar concerns are now being raised much closer to home. In the UK, ongoing legal action involves rugby union, rugby league and football governing bodies, with over 1,000 former players seeking compensation. They claim they were not properly informed of, or protected from, the long-term risks to their brain health associated with repeated head impacts. High-profile former internationals such as Steve Thompson MBE and Alix Popham have since been diagnosed with probable CTE and early-onset dementia, bringing renewed attention to the issue.
However, CTE is only one part of a much broader conversation. Repeated concussions, sub-concussive impacts, and single traumatic brain injuries can all lead to long-term physical, cognitive and emotional changes. Many people living with traumatic brain injury (TBI) or acquired brain injury will never develop CTE, yet still face significant, lifelong challenges that deserve recognition, understanding and support.
So, what exactly is CTE — and how does it relate to the wider spectrum of brain injury?
Chronic Traumatic Encephalopathy, or CTE, is not a new condition. It was first described in 1928 in boxers, who were then called “punch-drunk” (Martland, 1928). Today, we know CTE is a progressive brain disease linked to repeated head trauma. While it was once thought to be caused only by concussions, research now shows that repetitive mild head impacts, even those that don’t cause obvious symptoms, can also lead to CTE. This means it’s been found not just in athletes, but also in military personnel, victims of domestic violence, and others with repeated head injuries.
Repeated trauma causes abnormal build-up of a protein called Tau. Normally, Tau helps stabilize microtubules — tiny tubes inside neurons that transport nutrients and molecules. But when Tau is damaged by repeated trauma, it can form clumps called neurofibrillary tangles. These tangles disrupt how neurons work and can lead to cognitive decline. The abnormal form of Tau is often referred to as p-Tau.
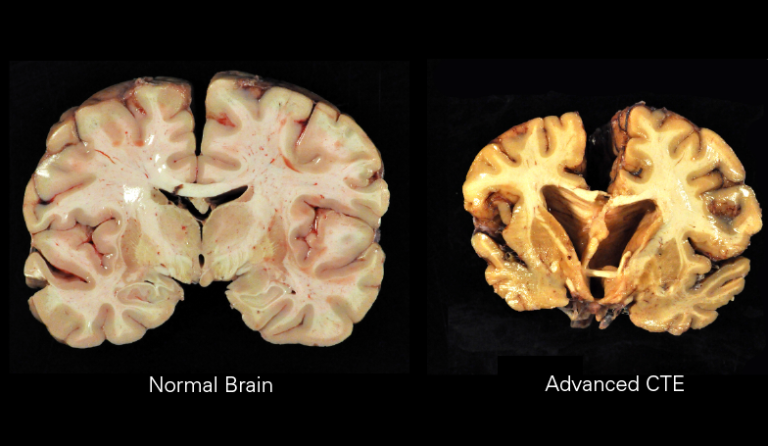
Trauma can also cause neuropil threads — microscopic abnormal structures in the brain’s grey matter that interfere with neuron function. Over time, these changes accumulate, and the pattern of Tau build-up in CTE is distinct from other diseases like Alzheimer’s. For example, in early CTE, p-Tau clusters appear in the surface layers of the brain’s grey matter, often near small blood vessels. In later stages, larger-scale changes occur, including shrinkage of grey and white matter, and damage to key areas like the thalamus, hypothalamus, and hippocampus.
Researchers led by McKee have described four stages of CTE:
Stage I: Small, isolated p-Tau clusters in the cerebral cortex.
Stage II: Multiple p-Tau clusters in the frontal, temporal, and parietal lobes.
Stage III: Degeneration in the medial temporal lobe, including the hippocampus and amygdala, with p-Tau around blood vessels.
Stage IV: Severe p-Tau spread throughout the brain, brainstem, cerebellum, and sometimes the spinal cord.
Studies show that symptoms of CTE often appear around 14–15 years after retirement from sport or repeated head trauma. The severity of symptoms and brain changes is linked to how long someone has been exposed to concussions or repeated sub-concussive hits (McKee, 2013).
Symptoms and Diagnosis of CTE
Chronic Traumatic Encephalopathy (CTE) is a progressive neurodegenerative disease associated with repeated head impacts, including concussions and sub-concussive blows. It has been identified in individuals involved in contact sports, military service, and other environments where repetitive brain trauma occurs.
CTE develops over time and may not present symptoms until years — sometimes decades — after the initial injuries.
What Causes CTE?
CTE is believed to be caused by repeated head trauma, rather than a single concussion. This includes:
- Multiple diagnosed concussions
- Sub-concussive impacts (blows to the head that do not cause obvious symptoms)
- Repetitive collisions in contact sports
- Blast exposure in military settings
- Ongoing physical trauma to the head in domestic violence
Over time, repeated trauma is thought to trigger abnormal changes in the brain, including the build-up of a protein called phosphorylated tau (p-Tau). These abnormal protein deposits interfere with normal brain function and are a defining feature of CTE.
Symptoms of CTE
Because repeated concussions and sub-concussive impacts can affect many different areas of the brain, symptoms can vary widely from person to person in both type and severity.
Common symptoms include:
Cognitive Symptoms
- Memory loss
- Difficulty concentrating
- Slowed thinking
- Problems with planning and decision-making
Behavioural Symptoms
- Irritability
- Impulsivity
- Aggression
- Personality changes
Emotional Symptoms
- Depression
- Anxiety
- Mood swings
- Low motivation
The Stages of CTE
Research led by Dr. Ann McKee has identified four pathological stages of CTE. The symptoms of CTE are closely linked to these stages:
Stage I:
Often no symptoms, or mild memory problems and low mood.
Stage II:
Behavioural changes, irritability, and more severe depression.
Stage III:
Cognitive difficulties, including memory loss and trouble with planning or decision-making.
Stage IV:
Advanced problems with language, thinking, movement, and sometimes psychotic symptoms.
It is important to note that not everyone will follow the same pattern, and progression can vary.
Can CTE Be Diagnosed?
Currently, there is no way to definitively diagnose CTE in a living person. The characteristic brain changes — including p-Tau deposits — can only be seen under a microscope after death.
However, researchers have developed criteria for Traumatic Encephalopathy Syndrome (TES) to help identify individuals likely to have CTE while alive.
TES considers four key factors:
- A history of repeated head impacts.
- Core symptoms of cognitive difficulties and/or behavioural changes.
- Progressive worsening of symptoms over time.
- Symptoms that cannot be fully explained by other medical or psychiatric conditions.
Functional impact is assessed on a scale from fully independent to severe dementia (Katz, 2021). While TES is currently a research tool, it may help doctors better understand and eventually diagnose CTE in living patients.
Why Awareness Matters
Because CTE cannot currently be confirmed during life, prevention and early recognition are critical. Understanding the long-term risks of repeated head trauma allows individuals, families, and sporting organisations to make informed decisions.
At Marshalling Brain Injuries Alliance, our mission is to raise awareness of the long-term risks of repeated head trauma, particularly in contact sports. We advocate for education, prevention, and informed decision-making to protect future generations.
If you have a history of repeated head impacts and are experiencing symptoms such as memory changes, mood difficulties, or behavioural changes, we strongly encourage you to seek medical advice and ensure your healthcare provider is aware of your brain trauma history.
You are not alone — and support is available.
CTE: Myths & Facts
There is a lot of confusion and misinformation surrounding Chronic Traumatic Encephalopathy (CTE). Understanding the facts is essential for prevention, early recognition, and reducing stigma.
Why Facts Matter
Understanding the reality of CTE helps reduce fear, stigma, and misinformation. It also encourages informed decisions about brain health and empowers individuals to seek support early.
At Marshalling Brain Injuries Alliance, we are committed to sharing trusted, evidence-based information — because knowledge protects lives.
Myth 1:
CTE only affects professional athletes.
Fact:
CTE has been identified in individuals from a range of backgrounds, including amateur athletes, military veterans, and others exposed to repeated head impacts. It is not limited to elite sport — repeated trauma at any level may increase risk.
Myth 2: You must have had diagnosed concussions to develop CTE.
Fact:
Research suggests that repeated sub-concussive impacts — blows to the head that do not cause obvious concussion symptoms — may also contribute to the development of CTE. It is cumulative exposure that appears to matter most.
Myth 3:
One concussion causes CTE.
Fact:
CTE is associated with repeated head trauma over time. A single concussion does not automatically mean someone will develop CTE.
Myth 4: CTE can be diagnosed with a brain scan.
Fact:
There is currently no scan or blood test that can definitively diagnose CTE in a living person. Diagnosis can only be confirmed after death through examination of brain tissue. Clinical criteria such as Traumatic Encephalopathy Syndrome (TES) are used to guide understanding during life.
Myth 5: Mood changes after brain injury are just “personality issues.”
Fact:
Mood swings, depression, irritability, and impulsivity can be neurological symptoms linked to brain injury. These changes are medical in nature — not character flaws.
Myth 6: Nothing can be done if someone has suspected CTE.
Fact:
While there is currently no cure, symptom management, rehabilitation, mental health support, and lifestyle interventions can significantly improve quality of life. Early support makes a difference.
Myth 7: Talking about CTE damages sport.
Fact:
Raising awareness protects athletes. Education around concussion protocols, safe return-to-play decisions, and long-term monitoring strengthens sport and prioritises player wellbeing.
Are you experiencing a mental health crisis?
There is help for you!
Shout: For 24/7 text support, text SHOUT to 85258 or click HERE
NHS 111 Online or Phone: If it's not an emergency but you need urgent help with your mental health, you can access NHS 111 online or by calling 111
Samaritans: Call 116 123 to talk , or email: jo@samaritans.org for a reply within 24 hours or click HERE
CALM - 0800 585 858 or click HERE
Mind - 0300 1233 393 or click HERE
No Panic - 0844 9674 848 or click HERE
National Domestic Abuse - 0808 2000 247 or click HERE